Effect of hyperventilation on arterial oxygen saturation during exercise
Wood, R.J. and Morton, A. R., 'Effect of hyperventilation on arterial oxygen saturation during exercise', Report to the Australian Sports Commission, Applied Sports Research Program, 1997.
Lowered arterial blood oxygen saturation (SaO2) occurs in approximately 50% of highly-trained (HT) endurance athletes during exercise (Powers et al., 1988; Martin et al., 1992a). There are several mechanisms within the pulmonary system which can cause a decrease in Sa02 (Powers et al., 1993), one of these being an inadequate hyperventilatory response to exercise (Dempsey et al., 1984). Several studies have found evidence for this (Miyachi & Tabata, 1992; Caillaud et al., 1993; Harms & Stager, 1995; Turcotte et al., 1997), while others have not (Powers et al., 1992). The role which VE plays in causing desaturation during exercise is still not clear and has not been investigated fully.
 By whatever mechanism SaO2 level is decreased, the effect may be exacerbated in the presence of relatively low exercise ventilation causing a lowered driving force for O2 across the alveolar to capillary membrane. Conversely, desaturation may be prevented by increasing VE, which would consequently increase the CO2 concentration gradient from the alveoli to pulmonary capillaries and therefore O2 transfer into the blood. Although it is not believed to be in widespread use, there is anecdotal evidence of athletes from some eastern block countries using hyperventilation breathing techniques to enhance performance (The Age, 1992). This has been supported by experimental studies that have increased VE and subsequently demonstrated increases in SaO2. Norton et al., (1995), showed an increase in VE of 15.7 l from maximal to supra-maximal exercise, and subsequently SaO2 increased from 93.2 to 94.2%. In other studies, subjects breathing a helium-oxygen gas mixture during exercise increased VE, causing a subsequent increase in SaO2 (Dempsey et al., 1984; Powers et al., 1986). However, no studies have investigated the effect of voluntary increases in VE on SaO2 levels. Voluntary hyperventilation can easily be performed in the competitive situation by the athlete, and therefore is potentially a practical method of counteracting desaturation and improving performance.
By whatever mechanism SaO2 level is decreased, the effect may be exacerbated in the presence of relatively low exercise ventilation causing a lowered driving force for O2 across the alveolar to capillary membrane. Conversely, desaturation may be prevented by increasing VE, which would consequently increase the CO2 concentration gradient from the alveoli to pulmonary capillaries and therefore O2 transfer into the blood. Although it is not believed to be in widespread use, there is anecdotal evidence of athletes from some eastern block countries using hyperventilation breathing techniques to enhance performance (The Age, 1992). This has been supported by experimental studies that have increased VE and subsequently demonstrated increases in SaO2. Norton et al., (1995), showed an increase in VE of 15.7 l from maximal to supra-maximal exercise, and subsequently SaO2 increased from 93.2 to 94.2%. In other studies, subjects breathing a helium-oxygen gas mixture during exercise increased VE, causing a subsequent increase in SaO2 (Dempsey et al., 1984; Powers et al., 1986). However, no studies have investigated the effect of voluntary increases in VE on SaO2 levels. Voluntary hyperventilation can easily be performed in the competitive situation by the athlete, and therefore is potentially a practical method of counteracting desaturation and improving performance.
The purpose of this study was to determine if desaturation can be prevented in highly-trained endurance athletes by voluntarily increasing VE. If successful, this would indicate the important role of an adequate ventilatory response during exercise in maintaining high SaO2 levels, while also leading to a practical method by which the athlete may be able to prevent desaturation and possibly improve performance.
The subject group comprised seven male competitive triathletes (age; 27 ± 3 years; height: 1.81 ± 0.06 m; mass 73.6 ± 7.3 kg), who volunteered to participate after previously achieving a decrease in SaO2 from rest of 5% or greater during a cycle VO2max test.
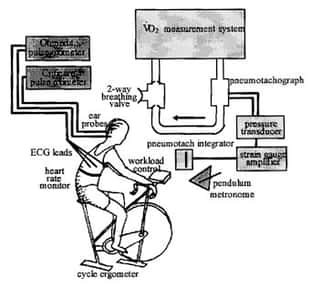
The subjects attended the laboratory for two testing sessions within a one month period. The first session was to determine the control VE level during a 6-minute submaximal cycle ergometer test (C). Also during this session, the subjects were able to practice using the biofeedback equipment to be used in the second session. The second session consisted of two 6-minute submaximal cycle ergometer tests, using biofeedback in each test to control VE. In one test the VE level as measured during C was mimicked (M), and in the other, the hyperventilation test (H), an attempt was made to increase VE by 20%. The M and H tests were conducted in a randomized order with a minimum of 30-minutes recovery between tests.
This study found that voluntary hyperventilation was able to reverse the decrease in SaO2 levels during high intensity constant load exercise. This is the first study to investigate the effect of voluntary hyperventilation on SaO2, though other studies have similarly been able to increase SaO2 by using exercise stimulus to increase VE (Norton et al., 1995), by manipulating PiO2 (Dempsey et al., 1984; Powers et al., 1989b), and increasing VE while breathing Helium-O2 mixture (Dempsey et al., 1984; Powers et al, 1986). The changes that were measured for VE and SaO2 were in proportion to the results in the study by Norton et al. (1995). They found an increase in VE by 10% corresponded to an increase in SaO2 of 1%, compared to the present study where a 15% increase in VE from C to H corresponded to a 1-5% increase in SaO2.
The effect of changes to SaO2 on VO2max or performance could not be determined in this study as the tests were performed at a constant workload, though increases in SaO2 have previously been shown to improve VO2max (Powers et al., 1989b; Pedersen et al,, 1992a). Powers (1989b) found that a decrease in SaO2 to 92-93% is sufficient to affect VO2max, and each 1% decrement in SaO2 below this level results in a 1% decrement in VO2max. These figures were determined through using hyperoxic breathing to increase SaO2 and VO2. In the present study, the increase in SaO2 from C to H was only small, though based on these results, the mean increase of 1,5% could improve VO2max by 1.5% if SaO2 was initially below 92-93%. Although the mean SaO2 was greater than 93%, individually some of the subjects had lower SaO2 levels, with 5 of the Low subjects reaching 92% SaO2 or less during the VO2max test, and 3 of the 7 reaching this level during the submaximal tests, with the lowest Sa02 being 91%. Therefore, the change in Sa02 for some subjects may have been able to benefit VO2max levels, though the effect would only be small. Such a change in VO2max could still be significant in sports that require a high percentage of VO2max to be maintained for extended periods, and at the elite level where very small differences in performance determines success. It is possible that the higher SaO2 measured for H was due to a change in the properties of the haemoglobin-/sub>O2 dissociation curve, and not an increase in the partial pressure of O2. One of the factors that influences the dissociation curve is blood pH.
As the subjects only reached moderate levels of desaturation in this study, it cannot be assumed that similar results would be found using subjects who desaturate to a greater extent. Very highly-trained athletes, who would achieve lower saturation levels, have their ventilation closer to maximum (Johnson et al., 1992) and therefore may be unable to increase VE as effectively as the subjects in the present study. However, previous studies have shown that significant desaturation occurs in HT athletes at submaximal workload and ventilation levels, beginning at 70% of VO2max (Powers et al, 1984; Pedersen et al., 1992b). The VE level during exercise in the present study did not reach maximal levels, and all subjects were comfortably able to increase VE by between 10 and 25%. Even following induced hyperventilation, the new ventilation level was still well below MW (VE/MW = 74.9%). In fact many subjects said that the H breathing level was not difficult to achieve, and in some cases they preferred it to the lower level.
It appears that some athletes choose a relatively low ventilatory level in the presence of desaturation, despite the potential to increase ventilation, which would prevent the desaturation occurring. Therefore, in the case of athletes who desaturate, the self-selected level of ventilation may not be optimal for maximal performance. The small difference in SaO2 measured must be considered with caution due to the accuracy of the measurement method. The indirect measurement of SaO2 by pulse oximetry is not as accurate as using the direct measurement of arterial blood, though in a paper by Mengelkoch et al. (1994), most studies reviewed found pulse oximeters gave valid and reliable measurements of SaO2 during exercise. Validation of the two oximeters used in the present study gave a correlation of 0.94, though the standard error of the estimate was 1.4%. The increase in SaO2 following hyperventilation in this study (1.5%) is similar to the random error of the SaO2 measurement, and therefore any conclusions that are made are limited by this.
In conclusion, hyperventilation was able to reduce desaturation in highly-trained athletes by 1.5%. This change in SaO2 was similar to the error of the measurement apparatus, and the level of desaturation was similar to the threshold level below which performance is affected, so the results should be interpreted with caution. However, irrespective of the absolute levels of SaO2 reached, these results show the potential for a hyperventilatory technique to improve SaO2 levels, and possibly performance. Also, this is significant as voluntary hyperventilation is a technique that could be self-administered by the athlete during competition.
Related Pages
- Full list of research papers by Rob Wood
- Breathing during Exercise — should you use your mouth or nose?
- Breath Holding Fitness Test
- Hypoxia Training


